
Forum Replies Created
-
AuthorPosts
-
-
2025-11-19 at 7:02 pm #52061
 Siriluk DungdawaduengParticipant
Siriluk DungdawaduengParticipantQ1. Given regulations like GDPR (“right to be forgotten”), can a blockchain technology based on immutability (the inability to delete) ever be fully compliant with healthcare privacy laws?
In my view, pure blockchain can’t fully comply with GDPR because its immutability prevents data from being deleted, which conflicts with the “right to be forgotten.” The most practical solution is to use a hybrid approach where actual patient data is stored off-chain, and the blockchain is used only for permissions and audit trails. This compromise allows healthcare systems to meet legal privacy requirements, even though it sacrifices some of blockchain’s original benefits. The paper also notes that this issue is still unresolved and requires further research.
Q2. Who do you think should control a patient’s digital health identity? The patient, the government, or a consortium of hospitals? What are the biggest risks of each model?
RISK:
Patient-controlled identity:
– Digital divide issue: Not everyone has smartphones or technical literacy (elderly patients, low-income populations)Government-controlled identity:
– Privacy concerns: Government surveillance of health data.
– If government system is hacked, everyone’s identity is compromised.
– What if government changes and misuses health data?Hospital consortium-controlled:
– Who decides who’s in the consortium? Creates the centralization blockchain was supposed to avoid.
– Patients might not trust hospital groups with this power.My opinion, A hybrid model makes most sense. Government issues a base digital health identity (ensuring universal coverage), patients hold their own keys but with recovery mechanisms (like multi-signature wallets where family members or trusted hospitals hold backup keys) and hospital consortiums manage the technical infrastructure and interoperability standards.
-
2025-11-19 at 6:50 pm #52060Siriluk DungdawaduengParticipant
1) How does this study challenge the traditional use of weather-station data (temperature) in vector models?
From what I understood after reading the paper, this study really challenges the common assumption that weather-station temperature represents the actual conditions mosquitoes experience. Traditionally, vector models use ambient temperature from weather stations because it’s easy to access and standardized. But this paper shows that mosquitoes don’t actually live in the same temperature environment that weather stations record.
One thing that stood out to me is that mosquitoes spend a lot of time in microhabitats, especially storm drains. And the study shows that temperatures inside storm drains can be very different from ambient temperatures—often warmer, especially in winter. Because of this “thermal insulation,” mosquitoes survive winter far better than models based on weather-station data would predict.
To me, this highlights a major problem:
– Traditional models may underestimate mosquito populations simply because they don’t account for microclimatic conditions where mosquitoes actually live.
– Another important point is the non-linear relationship between ambient and microclimatic temperature shown in the paper. This means we can’t just assume a simple linear adjustment or treat ambient temperature as a good proxy. (I’m not sure if I understand this part correctly, but to me it suggests that microclimate and ambient temperatures behave very differently across seasons and conditions.)
Overall, in my opinion, this study pushes us to rethink how we model mosquito populations.
If we keep relying only on weather-station data, we may be misjudging disease risk and designing control strategies based on incomplete environmental information.2) Only 8 out of 35 sensors produced complete data (27 lost due to theft and damage), what strategies could minimize sensor loss or damage if applied in ASEAN countries?
– Place sensors in less visible locations or disguise them as regular infrastructure components.
– Build strong relationships with local communities so residents feel ownership of the project and help protect the equipment.
– Work with village heads, community leaders, or even security guards who can keep an eye on the sensors.
– Check sensors frequently to catch and fix issues early.
– Use sensors that transmit data continuously, so you know immediately if one stops working.
– Use lower-cost sensors so losses are less financially devastating, allowing for wider deployment.I don’t have much background in this area, so if there is any part I’ve misunderstood, please feel free to suggest me. Thank you! 😊
-
2025-11-09 at 1:34 pm #51887Siriluk DungdawaduengParticipant
Hi Nang Phyoe, Your malaria surveillance system is clearly presented with a strong rationale, well-defined case definition, and effective data flow. The focus on stakeholder involvement and system evaluation shows good planning and sustainability. To further improve, you may add real-time data reporting, GIS mapping for hotspot tracking, and regular data quality checks. Overall, it’s a well-designed system with strong potential to enhance malaria control efforts. 😊
-
2025-11-09 at 1:30 pm #51886Siriluk DungdawaduengParticipant
Hi Kevin, your presentation clearly shows a strong understanding of COVID-19 surveillance. The integration of passive, active, sentinel, syndromic, and event-based approaches is excellent and ensures timely detection. I like the use of digital tools for real-time reporting and your attention to legal, ethical, and stakeholder collaboration. Including evaluation indicators also shows a commitment to improvement. You could further enhance it by showing how feedback loops work between local and national levels. Great job overall!
-
2025-11-09 at 1:27 pm #51885Siriluk DungdawaduengParticipant
Hi Wah Eah Lwin, Your presentation on the malaria surveillance system in Thailand is very informative and well-structured. I particularly appreciate how you linked the national malaria elimination goal (by 2026) with the rising trend of P. vivax and P. falciparum cases, which effectively highlights the urgency of strengthening surveillance. The inclusion of epidemiological data from the Ministry of Public Health makes the situation analysis clear and evidence-based.
I also like that your system design covers all essential components: objectives, legal basis, data flow, stakeholders, and evaluation indicators, which shows a solid understanding of surveillance frameworks. To further enhance your presentation, you might consider adding a visual dashboard or GIS mapping to show case distribution and transmission hotspots along the Thai-Myanmar border. This would make the data more engaging and support decision-making for targeted interventions. 😃
-
2025-11-03 at 10:30 am #51738Siriluk DungdawaduengParticipant
In my opinion, Prime Minister Lee Hsien Loong and President Donald Trump showed very different communication styles during the COVID-19 pandemic when viewed through the six principles of CREC.
I think PM Lee was a strong communicator. His speeches were clear, calm, and easy to understand. He avoided technical terms and explained the situation in a simple way. His messages were highly relevant, focusing on public concerns such as safety measures and government actions. He also showed empathy by acknowledging people’s fears and reassuring them, which helped reduce public anxiety. PM Lee provided good context by comparing Singapore’s situation with other countries, and his credibility came from using facts and maintaining a consistent, confident tone. Overall, his communication helped build public trust and a sense of stability.
In contrast, I think President Trump’s communication was less effective. Although he clearly announced major policies like the travel ban, some parts of his speech were vague and lacked explanation. His messages focused more on policy decisions rather than addressing people’s immediate concerns. I think he showed little empathy, as his tone was more formal and less reassuring. While he spoke with authority, some of his statements were later questioned by experts, which affected credibility. Moreover, his administration’s communication was often inconsistent, creating confusion among the public.
Comparing both leaders, I think the key difference lies in tone and focus. PM Lee emphasized empathy, clarity, and consistency, while President Trump focused more on authority and policy. However, both aimed to maintain public confidence during a crisis. Overall, PM Lee’s approach was more effective in connecting emotionally with the public and promoting trust, while President Trump’s approach showed strength in leadership but lacked the personal connection that helps people feel secure.
-
2025-10-27 at 3:03 pm #51601Siriluk DungdawaduengParticipant
After reading “The Evolution of Public Health Emergency Management” (Rose et al., 2017), I think Thailand has made progress in digital health development, especially in disease surveillance and communication systems. However, there are still areas that need improvement to strengthen our preparedness for future pandemics.
One theme that still needs more attention is the integration of information systems and data sharing across different sectors. The article emphasized the importance of information collection, integration, and sharing as a key domain of public health emergency management. In Thailand, health data often remain fragmented between hospitals, laboratories, and public health agencies, which can delay timely decision-making during emergencies. Improving this interoperability through standardized digital platforms and real-time data exchange would make our response faster and more coordinated.
Another area that could be strengthened is training and evaluation. Rose et al. (2017) mentioned that building staff competencies and continuously evaluating emergency management systems are essential. Although Thailand conducts simulation exercises, more consistent training programs that combine digital tools and field response could improve readiness, especially at the local level.
Overall, enhancing digital integration, capacity building, and evidence-based evaluation would help Thailand align better with international standards and be more resilient in future health crises. 😃
-
2025-10-27 at 2:48 pm #51600Siriluk DungdawaduengParticipant
1. Which outbreaks were declared as PHEIC?
From what I read in the documents, WHO has declared these major ones:2009 H1N1 (Swine Flu) – This was declared in April 2009 and lasted until August 2010
2014 Polio – Still ongoing actually, they reassess it every 3 months
2014 Ebola in West Africa – This was really serious – over 28,600 people infected and 11,325 deaths before it ended in 2016
2015-2016 Zika virus – Lasted about 10 months
2018-19 Ebola in Kivu – Another Ebola outbreak, ended in June 2020
COVID-19 – Obviously we all know about this one!2. Why do these outbreaks raise such concerns?
So basically, for something to become a PHEIC, it needs to meet at least 2 out of 4 criteria:Is it causing serious public health impact?
Is it unusual or unexpected?
Can it spread internationally?
Will it affect trade or travel?Like with H1N1, it spread super fast across borders. Ebola had those scary high death rates and needed help from multiple countries. Zika was linked to birth defects which freaked everyone out. These weren’t just local problems – they affected multiple countries and needed coordinated international responses.
3. What do I think could be the next PHEIC?
Honestly? I’m worried about antibiotic-resistant bacteria – like those “superbug” infections we keep hearing about.Here’s my reasoning:
They’re getting more common and scarier – some bacteria now resist ALL available antibiotics. That’s terrifying! They spread easily through hospitals, travel, and even through our food supply. And if we can’t treat basic infections anymore, even minor surgeries could become life-threatening.I’d also keep an eye on diseases spreading because of climate change. As the planet warms up, mosquitoes and ticks are moving into new areas where they’ve never been before. We might see dengue or malaria popping up in places that never had to deal with them.
What do you guys think? Do you agree, or do you see other threats we should be watching out for? 😃
-
2025-10-20 at 4:08 pm #51498Siriluk DungdawaduengParticipant
Omoleke and de Kiev’s evaluation revealed that the AEFI surveillance system in Kebbi State had major weaknesses affecting sensitivity and representativeness. From a public health perspective, I think the most serious design limitation is under-reporting due to passive surveillance and limited stakeholder participation. Many healthcare workers may not recognize or report all AEFI cases, especially from peripheral or private facilities.
To address this within six weeks, I would introduce targeted active case finding in a few sentinel sites combined with short refresher trainings and supervision visits. This would quickly raise awareness, improve reporting completeness, and provide data to benchmark sensitivity.1. Key design limitation and short-term action
Limitation: Reliance on passive reporting → high risk of missed AEFI cases.
Action: Conduct a six-week rapid active surveillance at selected high-volume sites and cross-check facility records against AEFI reports.
Rationale: This can estimate under-reporting and improve representativeness without redesigning the whole system.
2. Low-cost intervention to increase sensitivity
Using CDC surveillance attributes, one low-cost intervention could be:
Intervention: Implement a simple WhatsApp-based AEFI notification group for frontline health workers.
Expected trade-offs:
↑ Sensitivity and timeliness
↓ Data completeness and risk of unverified reports (false positives)
Indicators to track impact:
Number of AEFI reports submitted per month (baseline vs post-intervention)
Proportion of reports verified within 72 hours
Number of facilities actively contributing reports
This approach builds on simplicity and communication—two attributes already identified as partial strengths.
3. Broadening case definition for new vaccine
In my view, temporarily broadening the case definition makes sense at the start of a new vaccine introduction because early detection of unexpected signals is crucial.
Yes: It should be broadened initially to capture any unusual reactions.
Trigger to revert: After about two to three months or once the background AEFI rate stabilizes and no new safety signals emerge, the definition can revert to the standard one to avoid overburdening the system.
If the system capacity is already low, over-reporting could create false alarms—but early vigilance outweighs that short-term burden.
-
2025-10-20 at 11:50 am #51494Siriluk DungdawaduengParticipant
I think information technology really makes outbreak investigation much more efficient and accurate. In the past, everything relied on paper and manual reports, which took a long time. But now, with digital tools, each step can be done faster and more collaboratively.
For example:
During data collection, mobile apps or online systems help health workers report new cases instantly, which supports real-time monitoring.
For data analysis, software like GIS or R can visualize maps, show hotspots, and detect patterns that would be hard to see manually.
In communication, platforms like cloud storage or video meetings allow health teams and authorities to coordinate quickly, even from different locations.
For public communication, official websites and social media can share prevention messages and outbreak updates directly with the community.
Overall, I believe IT doesn’t just make the process faster, it also improves decision-making and collaboration among public health teams, which is essential for effective outbreak control.
-
2025-10-09 at 1:53 pm #51243Siriluk DungdawaduengParticipant
One digital technology from the article that I found most interesting is digital contact tracing using Bluetooth-enabled smartphone apps, such as TraceTogether in Singapore.
These apps automatically record when two users are near each other by exchanging anonymous Bluetooth signals. If someone later tests positive for COVID-19, the system can quickly alert all recent contacts so they can self-isolate or get tested. This reduces the delay and human error found in manual contact tracing, helping to stop the spread of the virus more effectively.
In my opinion, this technology had a significant impact during the pandemic. It showed how data and connectivity can strengthen public-health responses when used responsibly. Although challenges like privacy concerns and limited user adoption remain, I believe digital contact tracing has changed the way societies think about using technology for collective health protection.
-
2025-10-08 at 4:07 pm #51217Siriluk DungdawaduengParticipant
1. How can surveillance help to detect and control the disease?
I think surveillance helps us detect outbreaks early, keep track of how diseases spread, and plan better public health actions. It also shows where diseases are more common, which groups are most at risk, and whether things like mosquito control or vaccination programs are working well.
2. Should we conduct active or passive surveillance or both for the disease, why?
I think we should use both approaches together. Passive surveillance is cheaper and good for regular monitoring since it uses reports from hospitals or clinics. But during outbreaks, active surveillance is really important because it helps find cases that don’t go to health facilities and gives more accurate data. So, combining both methods would give us better coverage and help detect more cases.
3. Which method should be best to identify cases, why?
Laboratory-confirmed vs. Syndromic surveillance
I think lab-confirmed surveillance is more reliable since it gives accurate diagnosis. Syndromic surveillance is useful for early warning, but it’s not specific — it might include other illnesses. The best way is to use syndromic for quick alerts and confirm by lab later.Cases in medical facilities vs. community
Hospitals usually detect moderate to severe cases with full clinical data, while community surveillance can find mild or hidden cases. Combining both gives a better picture of disease spread and burden.Sentinel vs. Population-based surveillance
Sentinel sites are good for trend monitoring and save resources, but they may not represent the whole population. Population-based surveillance gives more complete data and helps estimate true incidence very useful for dengue in endemic areas.Case-based vs. Aggregated surveillance
Case-based data show individual details like age and location, which help in outbreak investigation. Aggregated data show only totals or trends. For dengue, case-based is better for targeted control.What dissemination tools for monkeypox surveillance information, and why?
I’d go with a mix of platforms.
– First, Health Alert Networks (HAN) are great for quick communication with doctors and public health teams.
– Then, online tools like ProMED or HealthMap give real-time global updates and maps — super useful for tracking outbreaks.
– Official government websites are important too since the data there are verified.
– And finally, social media helps spread information fast and raise public awareness. -
2025-08-26 at 1:50 pm #50140Siriluk DungdawaduengParticipant
As a hospital director, I would prioritize moving our hospital information system to cloud computing. This shift offers numerous benefits that align with our goals for efficiency, security, and patient care.
Cloud platforms provide scalable infrastructure, allowing us to manage increasing data volumes without heavy investment in physical servers. They also enhance accessibility, enabling authorized staff to securely access patient records from any location, which is vital for timely decision-making.
Additionally, cloud services offer robust data backup and disaster recovery, minimizing the risk of data loss. Security is another key advantage—leading cloud providers comply with healthcare regulations and implement advanced protection measures. Moreover, cloud computing supports integration with AI and data analytics tools, helping us improve diagnostics, resource management, and overall service quality. By adopting cloud technology, we can modernize our operations, reduce costs, and deliver better, more responsive care to our patients.
-
2025-08-18 at 5:27 pm #50053Siriluk DungdawaduengParticipant
Have you or your workplace ever been attacked by a cyber threat?
I have never personally experienced a cyberattack on my computer or during my tenure, I work in an organization that places strong emphasis on data management and computer security.What was the cause? How was your computer or data affected?
While I haven’t encountered a direct system breach, I did receive a suspicious email at work. The email appeared to be from a colleague, but upon closer inspection, the full email address was incorrect—an example of email spoofing, which is commonly used in phishing attacks. Fortunately, our company’s IT security policy includes training for all employees to recognize such threats. As a result, I did not open the link, and no damage occurred to my computer or data.What can you do to prevent it from happening again in the future?
To prevent such incidents, our organization enforces strict cybersecurity protocols, including:
– Regular staff training to enhance awareness of phishing and other threats.
– Implementation of a Disaster Recovery Plan (DRP) that outlines steps to recover critical IT systems and data in the event of a cyberattack.
– Routine software and security updates to patch vulnerabilities.
– Use of email filtering systems and two-factor authentication for secure access. -
2025-08-18 at 11:20 am #50026Siriluk DungdawaduengParticipant
I would build a mobile app for patients that connects with the hospital’s web-based system used by clinicians and staff. The app supports the pre-visit, visit, and post-visit workflow: patients can schedule appointments in advance, store key medical data such as drug allergies, and on arrival the app links to the hospital queue system to streamline check-in. For non-urgent conditions, patients can use telemedicine within the app, reducing travel costs, minimizing hospital crowding, and ensuring continuity of care. After consultations, the app integrates with the pharmacy system to allow home delivery of medications with real-time tracking and follow-up reminders.
I would choose a mobile app (patient-facing) combined with a web app (hospital-facing) instead of a LAN client/server solution because mobile and web are accessible, scalable, and interoperable with existing hospital systems.
To ensure data security, the app would apply end-to-end encryption, two-factor authentication, and role-based access controls to protect sensitive patient information. Compliance with standards such as HIPAA or equivalent national regulations would also be integrated. Regular data audits, secure APIs, and anonymization of non-essential data would further safeguard privacy.
This design improves medical outcomes by enabling timely access to care, reducing missed appointments, enhancing continuity of treatment, and improving medication adherence, while maintaining patient trust through robust data protection.
I’d be happy to hear your comments or ideas. 😊
-
2025-08-06 at 10:23 am #49930Siriluk DungdawaduengParticipant
I’d point to healthcare record management as a prime example of a system still facing significant challenges.
Healthcare facilities face significant challenges with fragmented patient information systems. Medical records remain scattered across providers, creating incomplete histories, duplicate testing, and coordination failures.
Problematic Components:
Data represents the primary challenge. Patient information exists in silos across paper records, incompatible electronic systems, and inconsistent formats, making critical information inaccessible when needed.Software issues include outdated, non-communicating Electronic Health Record systems and continued reliance on paper-based processes lacking integration capabilities.
Process inefficiencies force staff to spend excessive time on data entry and manual information transfers between systems, with no standardized sharing protocols.
People problems encompass inadequate training, resistance to change, overwhelming interfaces, and insufficient IT support.
Hardware limitations, while less critical, include outdated computers and unreliable network infrastructure affecting system performance.
Improvement Solutions:
– Implement interoperable EHR systems with standardized data formats
– Develop comprehensive staff training and change management programs
– Create streamlined workflows reducing redundant data entry
– Establish reliable data security and backup protocols
– Invest in user-friendly interfaces supporting clinical workflows -
2025-06-03 at 8:50 pm #48691Siriluk DungdawaduengParticipant
1) Did uploading your picture and presenting it in a shared virtual space feel different from sharing it in a classroom or discussion board? How so? Yes, it felt significantly different and more interactive, similar to walking through a real gallery. I could see the context of images in a 3D space, which created a different perception and understanding. I also felt more like part of a virtual community compared to traditional sharing methods. What I enjoyed most was being able to naturally walk around and view my classmates’ work in an organic way. However, I did need some time to adapt to the virtual environment, probably because I don’t frequently play games or use virtual environments like this.
2) Do you think virtual gallery spaces could be useful in real academic or professional settings? Why or why not? I believe virtual gallery spaces have significant benefits in academic environments in several ways:
– Art and Architecture Education: They can simulate museums or historical sites, providing access to places that might otherwise be unreachable.
– Research Presentations: They offer a more memorable experience compared to traditional presentation methods, making research more engaging and impactful.
– Collaborative Learning: Students can explore and discuss together in the same virtual space, fostering better interaction and knowledge sharing.
– In professional work environments, I think virtual galleries would be particularly beneficial for collaborative projects that require creativity and innovation. They could enhance teamwork by providing an immersive space where ideas can be visualized and shared more effectively than traditional meeting formats.3) Provide screen shots of your avatar with your uploaded picture and your two comments in this post.

-
2025-05-28 at 10:56 pm #48633Siriluk DungdawaduengParticipant
1. Your Personal Experience
Which apps or videos did you try with your headset?
I tested several applications with my Google Cardboard headset, including the Google Cardboard app, VR Space, VR Roller Coaster, and VR Jurassic.What did you enjoy most about the experience?
While I have previously used VR headsets, this experience was distinctly different as it was the first time I assembled a Cardboard device myself. The most exciting aspect was experiencing VR content through a device I had personally constructed. Among all the applications I downloaded and tested, VR Space was particularly engaging. I found it fascinating to explore the virtual space environment through my own handmade creation, which added a unique sense of accomplishment to the immersive experience.Were there any parts that didn’t work well or could be improved?
Several limitations became apparent during my testing. Many applications required payment to access their full features, with the premium versions offering superior visual quality and more engaging content compared to the free alternatives. Regarding the physical aspects of the self-assembled Cardboard, extended use resulted in mild dizziness and discomfort. This may have been exacerbated by wearing prescription glasses underneath the headset, though I am uncertain whether this significantly impacted the experience. In terms of interaction, I encountered difficulties with gesture-based controls—specifically, I was unable to perform head-nodding interactions as effectively as anticipated, which limited my ability to navigate certain applications intuitively.2. Connect to the Concepts from the Lecture
Did you experience stereoscopic vision? Why or why not?
Yes, I successfully experienced stereoscopic vision through the properly aligned lenses integrated into the Cardboard structure. The dual-lens system effectively created a three-dimensional visual experience by presenting slightly different images to each eye, allowing my brain to perceive depth and dimensional space within the virtual environment.Which psychological factors did you feel were active during your VR experience? Which ones were missing?
During my experience with VR Space, I felt a strong sense of engagement and genuine participation in the virtual environment. The application demonstrated effective immersion through responsive head tracking when I moved or rotated my head, the visual perspective adjusted accordingly, creating a compelling sense of presence within the space environment. However, several factors limited the full psychological impact of the experience. The realism was constrained by the visual limitations of free applications, which lacked the visual fidelity necessary for complete believability. Additionally, I encountered spatial boundaries that restricted exploration, preventing me from fully investigating the virtual space environment, which diminished the overall sense of presence and agency.Was there any interaction technique you used in the app? If not, what interaction methods would you have liked to see?
I successfully utilized head-tilt navigation to control movement within VR Space, which provided an intuitive method for exploring the virtual environment. However, the interaction experience would have been significantly enhanced with gaze control functionality, allowing me to select specific celestial bodies or locations for further exploration simply by directing my visual attention toward them. This would have provided more precise and intentional navigation capabilities, enhancing the overall user experience and sense of agency within the virtual space environment.
-
2025-05-24 at 11:03 pm #48593Siriluk DungdawaduengParticipant
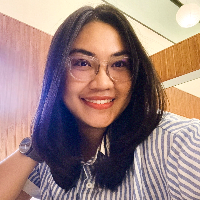
Visualization & Experimentation
https://snipboard.io/Jyzkfr.jpg

I conducted a temperature manipulation experiment using a hairdryer set to hot air mode directed at the sensor. This increased the temperature to 65.7°C and caused the humidity to drop to 9.4%. I then placed the sensor in an air-conditioned room and observed changes in both temperature and humidity displayed on the screen.
Challenges & Solutions
Initially, I encountered the error message “Failed to read DHT sensor!” in the Serial Monitor despite running the code several times. I suspected this was due to immersing the sensor too deeply in warm water, which caused the sensor board to become wet and unreadable. This moment was quite humorous, as our instructor had warned us about this beforehand. To address the issue, I dried the sensor board using a hairdryer on a normal setting, reconnected the USB to the computer, and uploaded the code again. I was thrilled when the sensor began functioning again.
However, I faced another challenge in Lab Part 2 when data failed to transmit to Google Sheets. After several attempts, I discovered the problem was due to an incomplete Wi-Fi name entry. I had entered only the base name without the “_2.4G” suffix, which was required for my network. Reading posts on the class forum and learning from classmates who shared similar issues helped me identify and correct the mistake. I am grateful for their contributions.
As someone whose regular work does not involve this kind of technical experimentation, I initially felt anxious about the lab. However, after engaging with the tasks, I found the learning process enjoyable and relevant.
Ideas for Improvement & Application
I really liked this application—it was manageable and easy to follow. Like some of my classmates, I would appreciate if the sensor were waterproof. I found it fun to experiment with immersing the sensor in both hot and cold water. However, after the sensor stopped functioning due to water exposure, I became hesitant to continue experimenting in that way. -
2025-05-12 at 10:07 pm #48499Siriluk DungdawaduengParticipant
Article Selection: “A novel framework for a remote patient monitoring (RPM) system with abnormality detection”
Authors: Chia-Rong Su, Jeyhun Hajiyev, Changjui James Fu, Kuo-Chin Kao, Chih-Hao Chang, Ching-Ter Chang
Citation: https://doi.org/10.1016/j.hlpt.2019.05.008Summary:
This research introduces an advanced Remote Patient Monitoring (RPM) system designed specifically for aging populations, leveraging Internet of Things (IoT) and Multi-Agent System (MAS) technologies. The framework provides an automated healthcare solution that can trigger medical alerts, medication reminders, hospital visit notifications, and social support mechanisms in real-time. By integrating various remote sensors and user devices, the system collects and analyzes patient data, transforming it into meaningful information that allows healthcare professionals to respond quickly and accurately. The study addresses critical challenges in modern healthcare, including rising costs, increasing chronic diseases, and a shortage of healthcare professionals. Implemented and simulated in a hospital intensive care unit setting, the system demonstrates the potential to improve patient care through advanced technological integration.Objective:
The primary goal of this IoT system is to create an effective, automated Remote Patient Monitoring (RPM) system that: Provides timely and precise medical support for aging populations, Enables autonomous functioning of patient monitoring, Facilitates secure and flexible healthcare information management and Automatically trigger medical interventions and support mechanisms.Sensors Used: The system incorporates multiple types of sensors, including:
• Vital sign monitoring sensors
• Environmental element sensors
• Patient behavior tracking sensors
• Communication and notification sensors
• Device management sensorsThe framework supports up to 250 communication protocols through Kepware’s KEPServerEX communication platform, allowing for extensive sensor integration and flexibility.
Challenges:
Key challenges during the development and implementation of the system included:
Technical Challenges:
o Integrating multiple communication protocols
o Ensuring secure data transmission
o Managing diverse sensor technologies
o Implementing reliable message routing
Logistical Challenges:
o Adapting to varying network conditions
o Supporting low-bandwidth and high-latency networks
Ethical Challenges:
o Protecting patient privacy
o Ensuring secure data transmission
o Developing an autonomous system with predefined action sets
o Maintaining patient confidentiality while enabling comprehensive monitoring -
2025-02-25 at 9:27 pm #47252Siriluk DungdawaduengParticipant
Thailand has committed significant investments across all dimensions of healthcare, including the expansion of services at every level. As a result, approximately four out of every five outpatient visits occur at community-based facilities. Despite these improvements, notable regional disparities persist, particularly between Bangkok and other regions.
The Thai healthcare system has evolved into a multi-tiered network, encompassing primary care services that provide basic medical treatment, health promotion, and disease prevention. These services are delivered through an extensive network of over 9,000 health stations located in every sub-district and approximately 700 community hospitals distributed throughout each district.
In addition, tertiary care facilities offer specialized treatment for complex conditions that require advanced medical equipment and expertise. This expansion has enabled the majority of outpatient services under the Ministry of Public Health to be accessed at local health centers and community hospitals. Nevertheless, inequities in hospital distribution remain, largely influenced by the socioeconomic potential of each region. For example, in Bangkok, private hospitals represent nearly two-thirds of all facilities, while the central region has approximately 30 percent private ownership. Moreover, the ratio of hospital beds per capita varies considerably, indicating persistent disparities in healthcare accessibility. These challenges necessitate comprehensive ongoing policy reform initiatives.
One widely examined case in the realm of primary health care interventions in Thailand is the Universal Health Coverage scheme, initiated in 2001. This program was designed to ensure equitable and comprehensive primary health care services for all population groups through investments in infrastructure, the widespread distribution of health facilities such as health centers and community hospitals and the enhancement of primary care personnel capacity.
The program’s success is evidenced by the substantial increase in service accessibility, with data indicating that approximately four out of every five outpatients under the Ministry of Public Health receive care within their communities. Moreover, strong governmental support and the implementation of clear policies to extend community-based services have been pivotal in achieving these outcomes.
Nevertheless, challenges persist in certain regions, particularly in rural or economically disadvantaged areas, where primary care interventions face obstacles such as uneven resource allocation, a shortage of qualified personnel, and unsystematic management practices. These issues contribute to regional disparities in health service accessibility, underscoring that despite the overall achievements, the primary health care intervention continues to encounter significant challenges that necessitate ongoing improvement.
-
2025-02-18 at 11:23 pm #47071Siriluk DungdawaduengParticipant
(1) Social Security Scheme (SSS) in Thailand
SSS covers private-sector employees through a compulsory payroll tax system (with contributions from employers, employees, and the government). It uses capitation payments to control costs and provides a defined set of benefits for both outpatient and inpatient care.Strengths:
– The tripartite funding mechanism helps maintain financial sustainability.
– Generally more cost-efficient than the CSMBS due to its controlled benefit structure and payment methods.Weaknesses/Challenges:
– Benefit levels are often lower than those under the CSMBS, which can result in disparities in service quality and access.
– There can be challenges in fully covering dependents or extending protection to informal workers, contributing to gaps in universal coverage.
– Integration with the UCS can be fragmented, leading to inequities across schemes.Needed Improvements:
– Harmonize benefit packages and payment systems between SSS and UCS to minimize inequities.
– Broaden the coverage to include dependents and vulnerable groups within the private sector.
– Enhance monitoring and quality assurance measures to ensure consistency of care.(2) Civil Servant Medical Benefit Scheme (CSMBS) in Thailand:
CSMBS provides very generous, comprehensive benefits for government employees, their dependents, and retirees. Its broad benefits package ensures access to a wide range of services and high-quality care.Strengths:
– High level of benefits and provider choice.
– Stability and strong political support for this group.Weaknesses/Challenges:
– Funded through general taxation with a fee‐for‐service payment model, it results in very high per capita expenditures and can drive overutilization.
– Cost containment is limited, making the system vulnerable to escalating costs and inefficiencies.Needed Improvements:
– Transitioning toward alternative payment methods (such as capitation or diagnosis-related groups) to help control costs.
– Strengthening auditing and information systems to reduce overuse and curb inefficiencies. -
2025-02-10 at 10:13 pm #46875Siriluk DungdawaduengParticipant
Thailand’s healthcare landscape reveals stark disparities between rural and urban settings. Urban areas like Bangkok boast advanced medical facilities, specialized healthcare professionals, and comprehensive medical technologies. Conversely, rural regions struggle with limited healthcare infrastructure, scarce medical professionals, and reduced access to quality healthcare services.
Key differences include:
– Physician density: Urban areas have 3-4 times more doctors per population
– Medical technology availability
– Specialized treatment options
– Healthcare infrastructure qualityInnovative solutions emerging include:
– Telemedicine platforms connecting rural patients with urban specialists
– Mobile health clinics reaching remote communities
– Digital health training programs for rural healthcare workers
– Community health worker empowerment initiativesPotential gap-closing strategies:
– Mandatory rural service rotations for medical graduates
– Financial incentives for healthcare professionals in underserved areas
– Enhanced telecommunication infrastructure
– Targeted rural healthcare investment
– Community-based healthcare training programsAddressing these disparities requires comprehensive, multi-sectoral approaches prioritizing equitable healthcare access.
-
2025-02-10 at 9:51 pm #46873Siriluk DungdawaduengParticipant
I want to share the health workforce situation challenges in Thailand:
– Uneven geographic distribution of healthcare professionals
– Rural areas experience severe healthcare worker shortages
– High concentration of medical professionals in urban centers like Bangkok
– Aging population increasing healthcare demand
– Limited professional development opportunities in remote regionsPotential Improvement Strategies:
– Implement targeted financial incentives for healthcare workers in underserved areas
– Develop comprehensive rural healthcare training and retention programs
– Create mandatory rural service rotations for medical graduates
– Invest in telemedicine infrastructure to extend healthcare access
– Enhance professional development and career progression opportunities in rural settings
– Increase healthcare worker salaries in remote regions
– Develop scholarship programs focused on recruiting professionals from underserved communitiesSpecific Recommendations:
1. Government should allocate dedicated funding for rural healthcare workforce development
2. Medical schools should integrate mandatory rural placement programs
3. Create competitive compensation packages for rural healthcare professionals
4. Develop specialized training programs addressing rural healthcare needsThese strategies could help address Thailand’s healthcare workforce disparities and improve overall healthcare accessibility across the country.
-
2025-01-27 at 5:35 pm #46809Siriluk DungdawaduengParticipant
I would like to give my view on point 4 from page 341: “A nonsignificant test result (P > 0.05) means that the test hypothesis is true or should be accepted.”
This point addresses the misconception that if a P value is greater than 0.05, it means the hypothesis being tested is true and should be accepted. However, a nonsignificant P value only suggests that the data are not unusual under the test hypothesis. It doesn’t prove the hypothesis is true. There could be other reasons for a large P value, such as a small sample size or other assumptions being incorrect. Therefore, it’s important to consider the context and other factors before concluding that the hypothesis is true.
-
2025-01-27 at 4:42 pm #46710Siriluk DungdawaduengParticipant
Using Electronic Medical Records (EMR) instead of traditional paper-based medical records has several advantages and disadvantages. Here are some key points to consider:
Advantages of EMR
1) Improved Efficiency:
• Quick Access: EMRs allow for faster retrieval of patient information, reducing time spent searching for records.
• Streamlined Workflow: Digital records streamline administrative tasks, such as scheduling and billing.
2) Enhanced Patient Care:
• Comprehensive Data: EMRs provide a complete view of a patient’s medical history, aiding in better diagnosis and treatment.
• Decision Support: Built-in alerts for drug interactions, allergies, and other critical information improve patient safety.
3) Data Accuracy and Security:
• Reduced Errors: Eliminates issues related to illegible handwriting and transcription errors.
• Secure Storage: Digital records are less prone to physical damage and loss compared to paper records.
4) Improved Coordination:
• Information Sharing: Facilitates easier sharing of patient information among healthcare providers, improving coordination of care.
• Remote Access: Allows authorized personnel to access records remotely, which is beneficial for telemedicine and consultations.Disadvantages of EMR
1) Initial Costs and Maintenance:
• High Upfront Costs: Implementing an EMR system requires significant investment in software, hardware, and training.
• Ongoing Maintenance: Continuous updates, technical support, and system maintenance can be costly.
2) Training and Adaptation:
• Learning Curve: Staff may need extensive training to use the new system effectively, which can be time-consuming.
• Resistance to Change: Some healthcare providers may be resistant to transitioning from paper to digital records.
3) Technical Issues:
• System Downtime: Technical glitches or system failures can disrupt access to patient records.
• Interoperability: Ensuring compatibility with existing systems and other healthcare providers’ EMRs can be challenging.
4) Privacy and Security Concerns:
• Data Breaches: Digital records are vulnerable to cyberattacks and data breaches, which can compromise patient confidentiality.
• Compliance: Ensuring compliance with data protection regulations requires robust security measures. -
2025-01-27 at 4:34 pm #46709Siriluk DungdawaduengParticipant
I would like to share some suggestions for coping with the challenges associated with using big health data in cardiovascular research and clinical care:
Missing Data
– Data Imputation Techniques: Use statistical methods to estimate and fill in missing values.
– Data Quality Improvement: Implement standardized data collection protocols to minimize missing data.
– Collaborative Data Sharing: Encourage data sharing among institutions to fill gaps.Selection Bias
– Random Sampling: Use random sampling techniques to ensure a representative sample.
– Propensity Score Matching: Match patients with similar characteristics to reduce bias.
– Sensitivity Analysis: Conduct sensitivity analyses to assess the impact of potential biases.Data Analysis and Training
– Training Programs: Offer training programs for healthcare professionals on big data analytics.
– Interdisciplinary Teams: Form teams with expertise in data science, statistics, and clinical care.
– User-Friendly Tools: Develop and use tools that simplify data analysis for non-experts.Interpretation
– Clear Guidelines: Establish clear guidelines for interpreting big data results.
– Expert Consultation: Consult with experts in data science and clinical care for accurate interpretation.
– Validation Studies: Conduct validation studies to confirm findings from big data analyses.Privacy and Ethical Issues
– Data Encryption: Use encryption to protect patient data.
– Anonymization: Anonymize data to protect patient identities.
– Ethical Frameworks: Develop and adhere to ethical frameworks for data use.
– Regulatory Compliance: Ensure compliance with data protection regulations (e.g., GDPR, HIPAA).Additional Suggestions
– Standardization: Standardize data formats and definitions to facilitate data integration and comparison.
– Collaboration: Foster collaboration between institutions, researchers, and policymakers to address common challenges.
– Patient Involvement: Involve patients in the research process to ensure their perspectives and concerns are considered. -
2025-01-27 at 4:17 pm #46707Siriluk DungdawaduengParticipant
I’d like to share my views on the four recommended points for public health professionals to fight corruption. Here they are, along with my thoughts:
1. Consensus Building: Engage stakeholders to agree on the scale and nature of corruption.
I agree with this recommendation. Building consensus among stakeholders is crucial because it ensures that everyone has a shared understanding of the problem. This collective agreement can foster a collaborative environment where all parties are committed to addressing corruption. It also helps in identifying the most pressing issues and prioritizing actions.2. Prioritizing Actions: Focus on the most impactful and feasible actions to address corruption.
I agree with this approach as well. By prioritizing actions, public health professionals can allocate resources more effectively and tackle the most significant issues first. This can lead to quicker, more noticeable improvements, which can build momentum and support for further anti-corruption measures.3. Holistic Approach: Use a multidisciplinary perspective to understand and tackle corruption.
I strongly agree with this recommendation. Corruption is a complex issue that often involves multiple sectors and disciplines. A holistic approach that includes legal, economic, social, and health perspectives can provide a more comprehensive understanding of the problem and lead to more effective solutions.4. Call to Action: Encourage a broader conversation about corruption in the health sector, emphasizing the need for political will and further research to develop effective policies.
I agree with this point. Raising awareness and fostering open discussions about corruption can help break the taboo around the topic. It can also mobilize political will and resources to address the issue. Additionally, further research is essential to develop evidence-based policies and interventions.Additional Suggestions
1. Transparency and Accountability: Implementing transparent processes and accountability mechanisms can deter corrupt practices. Regular audits, public reporting of health expenditures, and whistleblower protections can be effective measures.
2. Capacity Building: Training and educating health professionals on ethical practices and the importance of integrity can help build a culture of honesty and accountability.
3. Community Engagement: Involving the community in monitoring and reporting corruption can empower citizens and increase pressure on health systems to maintain high standards of integrity.
4. Technology Utilization: Leveraging technology, such as digital health records and e-governance platforms, can reduce opportunities for corruption by minimizing human intervention and increasing traceability.Overall, fighting corruption in health systems requires a multifaceted approach that includes both top-down and bottom-up strategies. By combining these recommendations with additional measures, public health professionals can create a more transparent, accountable, and effective health system.
-
2025-01-27 at 3:38 pm #46702Siriluk DungdawaduengParticipant
Example: Implementing an Integrated Health Data Repository to Enhance Care Coordination:
A regional healthcare network, consisting of several hospitals and primary care clinics, aimed to improve care coordination and patient outcomes by consolidating patient data into a single, integrated health data repository. Previously, each facility managed electronic health records (EHRs) independently, leading to fragmented data, duplication of tests, and gaps in patient information. By creating a centralized repository with secure data-sharing protocols, clinicians across the network gained real-time access to complete patient histories, laboratory results, and care plans.
Key Components of the Improvement
• Centralized Data Integration: Aggregation of clinical, laboratory, and radiology data into one platform.
• Advanced Analytics and Reporting: Automated alerts for abnormal lab results or potential drug interactions.
• Data Governance and Privacy: Clear guidelines on data access, usage, and storage to comply with regulations, Periodic audits to ensure data integrity and security.Possible Barriers to the Improvement Process
Interoperability and Technical Challenges
– Multiple Legacy Systems: Existing EHRs may use different standards, complicating data integration and requiring significant IT expertise.Financial Constraints
– Implementation Costs: Upfront expenses for software licenses, data migration, and staff training can be substantial.
– Ongoing Maintenance: Regular upgrades, system monitoring, and technical support add to long-term budget needs.Data Quality and Standardization
– Incomplete or Inconsistent Records: Poorly maintained legacy data can lead to errors or mistrust in the system if not cleaned and standardized.Privacy and Security Considerations
– Cybersecurity Risks: Centralized repositories can be targets for cyber-attacks if not properly safeguarded.By establishing a robust, integrated data repository and accompanying governance structures, healthcare networks can transform disjointed patient records into a unified, actionable resource. Although technical, financial, and organizational barriers can impede progress, strong leadership, comprehensive change management, and a focus on data quality can facilitate successful adoption and sustained improvement in care coordination and patient outcomes.
-
2025-01-06 at 8:12 am #46424Siriluk DungdawaduengParticipant
My name is Siriluk, you can call me ‘New’ 🙂
My background is in biotechnology and marketing, and I have worked in the clinical vaccine trial field for over seven years. I started my career as a Clinical Research Associate (CRA) in a pharmaceutical company, focusing on multiple site monitoring and clinical site management.
Driven by a passion for understanding the intricacies of clinical data management, I joined the data management team for clinical research studies in 2021. In this role, I contribute to ensuring the quality and accuracy of clinical trial data, utilizing my experience in trial coordination. My work often involves applying statistical principles to support data validation, monitoring, and reporting processes, ensuring compliance with regulatory standards and contributing to the success of clinical research projects.
-
2024-12-03 at 8:50 pm #46348Siriluk DungdawaduengParticipant
A comprehensive Disaster Recovery Plan (DRP) ensures organizational resilience by addressing key areas. Risk Assessment and Business Impact Analysis (BIA) identify critical systems, assess risks, and evaluate potential operational impacts. Clear Recovery Objectives, including Recovery Time Objectives (RTO) to minimize downtime and Recovery Point Objectives (RPO) to reduce data loss, are vital. Disaster Response and Activation procedures establish activation criteria and a robust communication plan to coordinate with stakeholders effectively.
Backup and Restoration Procedures define frequency and secure storage options (local, off-site, or cloud-based), while Replication and Redundancy ensure real-time database replication and system availability. Incident Management specifies roles, responsibilities, and recovery steps, complemented by regular Testing and Training to enhance preparedness. Cost-efficient Cloud Backups, Database Replication tools like SQL Server Always On, Virtualization, and Disaster Recovery as a Service (DRaaS) offer scalable recovery solutions. These strategies ensure compliance, scalability, and efficient implementation.
-
2024-12-01 at 6:04 pm #46335Siriluk DungdawaduengParticipant
In the clinical data management field, I propose a project idea based on the 12 steps of project management: “Transitioning from Paper-Based to Electronic Data Capture (EDC) in Clinical Trials.” This project aims to replace paper-based data collection with an EDC system to enhance data quality and streamline workflows. Objectives focus on data accuracy, efficiency, and compliance. Stakeholders, including sponsors, data managers, and site teams, are identified, and deliverables include a functional EDC platform and training materials. A detailed plan covers phases like system development, validation, and deployment, with allocated resources. Risks, such as user resistance, are mitigated, and progress is monitored. The project concludes with a review, documentation, and lessons learned session for long-term success.
-
2025-10-09 at 2:14 pm #51246Siriluk DungdawaduengParticipant
Hi Than Htike Aung, thank you for sharing your thoughtful insights. I agree with your points especially that combining both active and passive surveillance provides a balanced approach for effective dengue control, and that sentinel and case-based surveillance ensure high-quality, detailed data for early outbreak detection. I also support your idea of using public dashboards and epidemiological reports, as they enhance transparency, timely communication, and evidence-based decision-making. Thank you.
-
2025-10-09 at 2:09 pm #51245Siriluk DungdawaduengParticipant
Hi Wah Wah, thank you for sharing your opinion. I totally agree with your point about the use of social media platforms, as they serve as effective tools for rapid communication and allow the public to access real-time information. During the COVID-19 outbreak, I also observed how public health authorities used various social media platforms to communicate updates. Dashboards displaying daily case numbers, hospitalizations, and deaths were regularly shared, helping people stay informed. I also found it interesting to see flowcharts from different countries’ health departments that promoted preventive measures and clear public guidance. Thank you!
-
2025-10-09 at 2:01 pm #51244Siriluk DungdawaduengParticipant
Hi Than Htike Aung, thank you for sharing your opinion. I completely agree with the use of Bluetooth-based COVID-19 contact-tracing applications, as they enable rapid and comprehensive tracking of close contacts, which is highly suitable during an outbreak situation. This technology plays a crucial role in helping to stop the spread of infection.
I also checked out the additional information from the link you shared about Apple and Google partnering on COVID-19 contact tracing technology — it’s very interesting and informative. Thank you!
-
2025-08-18 at 4:09 pm #50048Siriluk DungdawaduengParticipant
Hi Sumitta, Thank you for sharing your experience. I agree with the points mentioned above. The identified problems clearly highlight critical gaps in software reliability, data quality, processes, and staff capability. The suggested improvements, such as upgrading software, standardizing data entry, providing clearer manuals, and training staff, are practical solutions that will enhance efficiency, accuracy, and overall healthcare service quality. 😊
-
2025-08-18 at 4:07 pm #50046Siriluk DungdawaduengParticipant
Hi Wah Wah, I agree with the points above. Effective use of Information Systems requires strong capacity building, standardized data management, and streamlined processes across the network. Software harmonization and hardware upgrades are also essential. Addressing these gaps will enhance collaboration, improve data-driven decision-making, and strengthen regional capacity in managing emerging health challenges. 😊
-
2025-08-18 at 4:04 pm #50045Siriluk DungdawaduengParticipant
Hi Sirithep, thank you for sharing your idea. I agree with your idea. Developing a mobile application for delivering laboratory results to both patients and doctors is highly beneficial. It promotes timely communication, enhances patient engagement, and improves adherence through reminders. This approach could reduce delays in care, support better treatment outcomes, and increase efficiency in healthcare delivery. 😊
-
2025-08-18 at 4:02 pm #50044Siriluk DungdawaduengParticipant
Hi Aung, Thank you for sharing your idea. I strongly agree with the idea. Developing a mobile app for chronic patient self-care is practical and impactful. Using local storage ensures privacy and cost efficiency, while HL7 FHIR enables seamless data exchange. Integration with smart devices also empowers patients to manage their conditions effectively, ultimately improving long-term health outcomes. 😊
-
2025-08-18 at 4:00 pm #50042Siriluk DungdawaduengParticipant
Hi Jenny, Thank you for sharing the current practices in the Philippines. I agree with you. The proposed app can greatly improve transparency between patients and hospitals by providing real-time updates and detailed explanations of medical expenses. This would not only help patients better understand their financial responsibilities but also reduce misunderstandings and conflicts, fostering trust in healthcare providers. 😊
-
2025-08-18 at 3:56 pm #50041Siriluk DungdawaduengParticipant
Hi Wah Wah, thank you for sharing your idea. I agree with your statement. Implementing a LAN client/server application in a hospital system is both practical and secure. It safeguards sensitive patient data through controlled access while ensuring fast communication. With strong security protocols and proper IT maintenance, this approach enhances workflow efficiency and supports improved medical outcomes. 😊
-
2025-06-03 at 9:00 pm #48693Siriluk DungdawaduengParticipant
Hi Aung Thura Htoo, Thank you for sharing your experience and your VR snapshot! I like your creative thinking regarding hybrid conferences and your consideration of accessibility for all users. The insight about the magnifying glass feature was particularly thoughtful!
-
2025-06-03 at 8:55 pm #48692Siriluk DungdawaduengParticipant
Hi Cing, Thank you for sharing your experience and your VR snapshot! Your perspective has definitely enhanced my own understanding of virtual learning environments!
-
2025-05-28 at 11:06 pm #48634Siriluk DungdawaduengParticipant
Hello Pacharapol, thank you for sharing your detailed VR experience with us. I completely agree with your observations! The interaction limitations are frustrating—gaze control like Fulldive’s approach seems more practical than awkward head tilting. Your point about glasses compatibility is spot-on; it’s a major design flaw. I also found mobile VR less thrilling than professional setups, confirming your Universal Studios comparison. Your insight about sense of gravity enhancing presence is excellent and directly supports lecture concepts about multisensory immersion in VR.
-
2025-05-12 at 10:29 pm #48502Siriluk DungdawaduengParticipant
Hello Chanapong, thank you for sharing this paper. this research is smart insoles could revolutionize healthcare by monitoring conditions like diabetes and Parkinson’s non-invasively. The potential to reduce hospital visits and catch early signs of health issues is incredible. It’s amazing how technology can transform medical diagnostics through something as simple as a shoe insert.
-
2025-05-12 at 10:26 pm #48501Siriluk DungdawaduengParticipant
Hello Abdillah, thank you for sharing the paper on the leverage of IoT PCT for pandemic disease detection, this IoT-based PCR system is groundbreaking! The portability and real-time data transmission could revolutionize disease monitoring, especially in remote areas. It’s fascinating how they’ve integrated multiple sensors to create a compact, efficient diagnostic tool with global health implications.
-
2025-05-12 at 10:16 pm #48500Siriluk DungdawaduengParticipant
Hello Tanatorn, thank you for sharing the paper on IoT-based health monitoring system offers innovative remote healthcare solutions, enabling real-time vital sign tracking for patients and elderly individuals. I think that it effectively addresses healthcare access challenges by leveraging wearable sensors, Arduino Uno, Raspberry Pi, and cloud technology to improve medical monitoring and patient care.
-
2025-01-27 at 3:51 pm #46704Siriluk DungdawaduengParticipant
Thank you for sharing. I agree with your assessment that, although the initiative focuses on crucial areas—service delivery, health workforce, and health information systems. There is a need for comprehensive enhancements across all WHO building blocks to fully meet objectives. Continued efforts in financing, medicine and technology, and governance will strengthen overall health system performance.
-
2025-01-27 at 3:44 pm #46703Siriluk DungdawaduengParticipant
Thank you for your sharing. Your explanation of Thailand’s “Cancer Anywhere” policy showcases its innovative design for delivering comprehensive cancer care. I fully concur that, while the policy promotes greater accessibility and equity, significant operational hurdles persist. Addressing these through better resource allocation, improved data sharing, and stronger leadership will be crucial for long-term success.
-
2025-01-06 at 10:18 pm #46428Siriluk DungdawaduengParticipant
Hi Thinzar 🙂 Thank you for your message.
It’s wonderful to learn about your extensive background in computer science, and software development, and your work in the health sector sounds fascinating. I’m particularly impressed by your focus on health information systems and your proficiency in SQL for data validation and reporting. These are valuable skills in ensuring the quality and usability of health data. 🙂
-
-
AuthorPosts
